てんかんの診療において発作の焦点の推測は重要と考えられます。
臨床的には発作時徴候など、様々な検査などを併用しててんかん焦点を推測していきます。
とくに薬剤抵抗性(難治性)の焦点性てんかんでは、焦点切除が治療選択肢として重要になってきます。
発作時徴候
前頭葉、側頭葉における発作時徴候に関しては以下のリンクから別の記事をご参照下さい。
また、側方徴候についても以下のリンクから別の記事をご参照下さい。
Insulo-opercular seizure
insular cortex(島皮質)とopercular cortex(弁蓋部)は、様々な発作徴候を示す。
その理由はinsula自体の機能が幅広いことと、様々な領域と機能的に連結しているからと考えられます。
Insulo-opercular seizureについて報告した論文では、以下のように分類しています。
・Group1 epigastric sensation and/or integrated gestural motor behaviors with or without feeling of fear or rage
領域:anteroventral insular regions and mesial temporal lobes
・Group2 auditory sensation and symmetric proximal/axial tonic signs
領域:posyeroventral temporal operculum
・Group3 orofacial and laryngeal signs
領域:intermidiate insulo-opercular regions
・Group4 somatosensory signs followed by nonintegrated gestural motor behaviors and/or asymmetric tonic signs
領域:posterodorsal insulo-opercular regions with propagation to the mesial frontal lobe
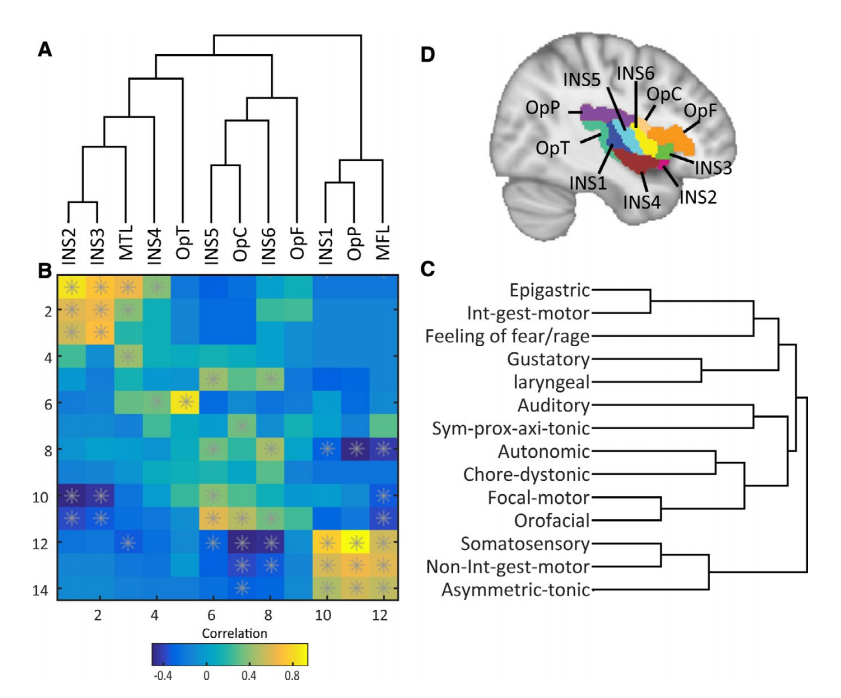
Epilepsia 2020;61:984-994から引用
てんかん焦点を推測するための領域
・Epileptogenic zone
この領域を切除することにより発作が消失する領域
・Irritative zone
発作間欠期にてんかん性放電が認められる領域
・Seizure onset zone
てんかん発作が始まる領域。発作時脳波(頭皮脳波・皮質脳波)により推察される。
・Ictal synptomatogenic zone
発作時に症状が出現する領域。てんかん性異常活動の伝播様式により、この領域は必ずしもEpileptogenic zoneとは一致しないことに注意が必要である。
臨床的な発作時の徴候は、この領域をみていることに留意する。
・Functional deficit zone
発作間欠期に神経学的、神経心理学的、脳機能画像などにおいて機能低下を示す領域

